When your breasts leak milk but you’re not pregnant or nursing, it’s not normal-and it’s not rare. About 20-25% of women experience this at some point in their lives. This isn’t just a weird side effect; it’s often a sign of something deeper: a hormone imbalance called hyperprolactinemia. And if left unchecked, it can stop your periods, make it harder to get pregnant, or cause anxiety that feels impossible to shake. The good news? We know exactly what causes it, how to test for it, and how to fix it-often in just a few months.
What Is Galactorrhea, Really?
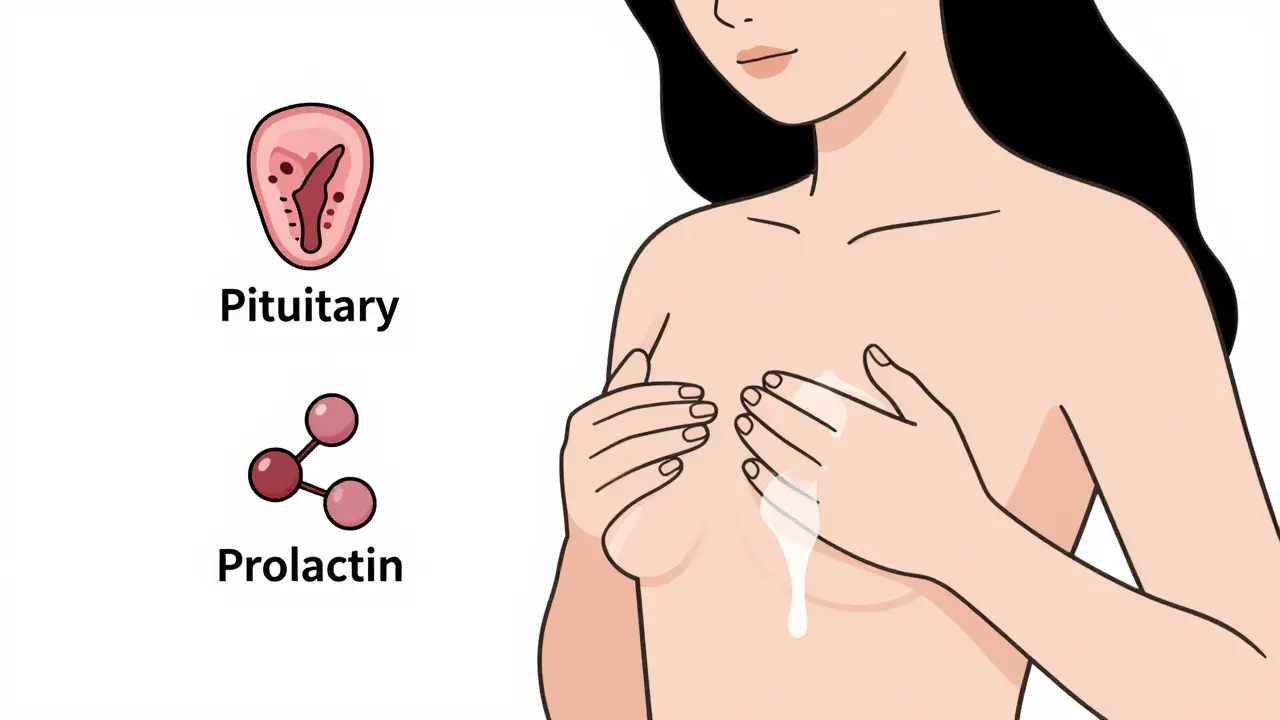
Galactorrhea is milky nipple discharge that happens outside of pregnancy or breastfeeding. It’s not a disease itself-it’s a symptom. And it’s usually bilateral, meaning both breasts are affected. About 70-80% of cases involve both sides. In 20-30% of cases, it’s only one breast, which can scare people into thinking it’s cancer. But cancer-related discharge is different: it’s bloody, watery, or brownish-not milky. If you’re seeing milk, it’s almost always hormonal.The trigger? Too much prolactin. This hormone, made in the pituitary gland, tells your body to make milk. Normally, it’s kept in check by dopamine, another brain chemical. But if something disrupts that balance-like a tumor, a medication, or even stress-prolactin spikes. Levels above 25 ng/mL are considered abnormal in non-pregnant women. Normal range? 2.8 to 29.2 ng/mL. So even a slight rise can cause trouble.
Why Does High Prolactin Cause Infertility?
Prolactin doesn’t just make milk. It also shuts down your reproductive system. High levels suppress GnRH, the hormone that kicks off ovulation. No GnRH? No estrogen surge. No estrogen surge? No egg release. That’s why women with hyperprolactinemia often stop getting their periods-sometimes for months or years. Studies show that 80-90% of women with this condition regain regular cycles once prolactin is brought back to normal.It’s not just about missing periods. Fertility drops because ovulation becomes unpredictable-or stops entirely. Men aren’t immune either. High prolactin can lower testosterone, reduce libido, and cause erectile dysfunction. But women are more likely to notice symptoms first because of the visible discharge and missed cycles.
What Causes Prolactin to Rise?
There are over a dozen reasons. The most common ones:- Prolactinoma: A benign tumor in the pituitary gland that overproduces prolactin. These are the #1 cause of high prolactin. Microprolactinomas (under 10 mm) are the most common-and they respond beautifully to medication.
- Medications: Antidepressants like SSRIs (sertraline, fluoxetine), antipsychotics (risperidone), and even some blood pressure pills can raise prolactin. Switching to bupropion or a different drug often fixes it.
- Hypothyroidism: When your thyroid is underactive, TSH rises and can accidentally trigger prolactin release. Simple blood tests catch this.
- Stress or nipple stimulation: Even a tight bra or chest wall injury can spike prolactin temporarily. That’s why doctors ask you to avoid breast exams or even tight clothing before a blood test.
- Idiopathic: In about 35% of cases, no cause is found. But that doesn’t mean it won’t resolve on its own-up to 30% of these cases clear up within a year without treatment.
That’s why diagnosis starts with more than just a prolactin test. You need thyroid function (TSH), kidney function (creatinine), and sometimes a pregnancy test-even if you’re sure you’re not pregnant. If prolactin is over 100 ng/mL, an MRI is recommended to check for a tumor. Below that? Often, doctors start with medication first.
Treatment: Cabergoline vs. Bromocriptine
The gold standard for treatment? Dopamine agonists. These drugs mimic dopamine, which tells the pituitary to stop pumping out prolactin. Two drugs dominate the market: cabergoline and bromocriptine.| Feature | Cabergoline (Dostinex) | Bromocriptine (Parlodel) |
|---|---|---|
| Dosing | 0.25-1 mg, twice weekly | 1.25-2.5 mg, daily |
| Effectiveness | 83% normalize prolactin in 3 months | 76% normalize prolactin in 3 months |
| Side Effects | Nausea (10-15%), dizziness | Nausea (25-30%), vomiting, low blood pressure |
| Cost (monthly) | $300-$400 | $50-$100 |
| Pregnancy Safety | Used safely during conception and early pregnancy | Historically preferred in early pregnancy |
| Long-Term Risk | Valve issues only at doses >2 mg/day for over a year | Minimal long-term risk at standard doses |
Most doctors start with cabergoline because it’s easier to take and better tolerated. One patient on Reddit said: “After 3 months on 0.5 mg twice a week, my discharge stopped and my period came back after 18 months.” That’s the norm, not the exception.
Bromocriptine is cheaper and has a longer safety track record in pregnancy, but nausea is a dealbreaker for many. One user wrote: “I had to take it at bedtime and still threw up twice a week for a month.” That’s why cabergoline now makes up 65% of the U.S. market for hyperprolactinemia treatment.
What About Surgery or Radiation?
For most people, medication is enough. In fact, 90% of small prolactinomas shrink or disappear within six months of starting cabergoline. Surgery is reserved for cases where:- The tumor is huge (>10 mm) and pressing on the optic nerve
- Medication doesn’t work or causes intolerable side effects
- The patient wants to get pregnant and refuses medication
Radiation is almost never used today. It’s slow, risky, and unnecessary when drugs work so well.
What If Treatment Doesn’t Work?
If prolactin stays high after 3-6 months of proper dosing, your doctor will check a few things:- Are you taking the medication correctly? Cabergoline is absorbed better on an empty stomach.
- Is another drug causing the problem? Review every pill, supplement, or herb you take.
- Is the MRI accurate? Sometimes small tumors are missed on standard scans.
- Is it really hyperprolactinemia? Rare conditions like kidney failure or liver disease can mimic it.
And don’t forget: some people have mildly elevated prolactin but no symptoms. Experts warn against treating those cases. One endocrinologist put it bluntly: “Overemphasizing prolactin levels without clinical correlation can lead to unnecessary treatment.” If you’re not having discharge, missed periods, or fertility issues, and your levels are only slightly above normal-you might not need anything at all.
What’s New in 2026?
The field is evolving. In January 2025, the FDA approved a new extended-release cabergoline that you take just once a week. Early trials show 89% effectiveness-better than the old version. That’s a game-changer for people who struggle with adherence.Novartis is testing a brand-new drug in phase 2 trials: a selective prolactin receptor blocker. Instead of lowering prolactin, it blocks the hormone from acting on breast tissue. That could mean no more milk-without touching the pituitary. Results are expected by late 2026.
Doctors are also moving toward team-based care. Mayo Clinic launched integrated endocrine-breast clinics in 2024. Patients used to wait 8 weeks for answers. Now? It’s down to 3.5 weeks. That’s faster diagnosis, fewer missteps, and less anxiety.
What Should You Do If You’re Experiencing This?
If you’re leaking milk and not pregnant:- Don’t panic. This is common and treatable.
- Stop squeezing or stimulating your breasts-this can make it worse.
- Write down every medication, supplement, and herb you take.
- See your doctor for a prolactin blood test and TSH check.
- If prolactin is over 25 ng/mL, ask about an MRI if it’s above 100 ng/mL.
- If you’re trying to get pregnant, mention it. Dopamine agonists are safe to use while conceiving.
Most people see results within weeks. Discharge stops. Periods return. Fertility comes back. And the anxiety? It fades with the milk.
Can galactorrhea cause breast cancer?
No, galactorrhea itself does not cause breast cancer. However, nipple discharge that is bloody, clear, or from one breast only can be a sign of cancer. Milky discharge from both breasts is almost always hormonal. If you’re unsure, a doctor may order a mammogram or ultrasound to rule out tumors.
Can I get pregnant while taking cabergoline?
Yes. Cabergoline is safe to use while trying to conceive and during early pregnancy. In fact, many women conceive naturally within months of starting treatment because ovulation returns. Doctors often continue the medication through the first trimester to keep prolactin low and prevent tumor growth.
How long does it take for prolactin levels to drop?
Prolactin levels usually start falling within days of starting medication. Most people see normal levels within 2-4 weeks. Discharge often stops in 1-3 weeks. But if you have a tumor, it may take 3-6 months for it to shrink noticeably.
Is galactorrhea common in men?
It’s rare, but it happens. About 1 in 10 cases of hyperprolactinemia occur in men. Symptoms include breast discharge, low libido, erectile dysfunction, or reduced body hair. Men are more likely to have larger tumors, so MRI is often recommended even at lower prolactin levels.
Can stress alone cause galactorrhea?
Yes. Severe physical or emotional stress can raise prolactin by 10-20 ng/mL, enough to trigger discharge in sensitive individuals. That’s why doctors ask you to rest before a blood test. If stress is the only cause, prolactin often normalizes on its own once the stressor is removed.
Do I need to take medication forever?
Not necessarily. If you have a small prolactinoma and your prolactin is normal for over a year, your doctor may try slowly reducing the dose. About 20-30% of patients can stop treatment without recurrence. But if the tumor was large or prolactin was very high, long-term or lifelong treatment may be needed.



11 Comments
bro prolactin is just nature’s way of saying you’re too stressed or eating too much soy
so let me get this straight… you’re telling me the solution to infertility is a pill that stops your body from making milk? what’s next, banning crying to fix depression?
the fact that we’re treating a physiological symptom like a bug to be eradicated instead of a signal from the body is so deeply western. prolactin isn’t the enemy-it’s the messenger. when we pathologize natural hormonal fluctuations without addressing root causes like chronic stress, sleep deprivation, or emotional suppression, we’re just medicating the symptoms of a broken system. i’ve seen women go from 80ng/mL to normal on cabergoline, but then relapse because their jobs, relationships, and self-worth are still in shambles. the pill fixes the lab result, not the life.
oh my god i had this after my mom died… no meds, just rest and chai tea for 6 months… and then it just stopped. i didn’t even know it was prolactin until i read this. thank you for saying it’s not cancer 😭
so you’re telling me the #1 cause of infertility is… a tiny brain tumor? and the cure is a pill you take twice a week? 🤯 i feel like i just won the medical lottery. also, why is this not on every women’s health podcast? this should be mandatory reading in high school. 🙏
the article says 35% of cases are idiopathic but ignores that most women with mildly elevated prolactin are overtested and overtreated. if you’re not symptomatic, stop chasing numbers. your endo is probably making commission off your MRI
in a nation where women are told to ‘just relax’ and ‘stop being so emotional,’ we now have a pharmaceutical fix for the very biology that society pathologizes. cabergoline isn’t medicine-it’s social control disguised as science. they’ll give you a pill to silence your body’s cries, but won’t give you paid maternity leave or mental health days. this isn’t treatment. it’s suppression with a prescription pad.
It is of paramount importance to acknowledge that the elevation of prolactin levels constitutes a neuroendocrine dysregulation, which may originate from a variety of etiologies including, but not limited to, pharmacological interference, hypothalamic-pituitary axis perturbations, and iatrogenic stimuli. The therapeutic efficacy of dopamine agonists is well-documented in peer-reviewed literature, yet clinical application must be individualized based on patient-specific biomarkers and symptomatology.
Thank you for writing this so clearly. I’m a guy and I didn’t even know men could get this. My cousin had it-no one told him it could be tied to his meds. He thought he was going crazy. I’m sharing this with him. 🙏
OMG I’ve been leaking milk for 2 years and thought I was broken. I stopped wearing sports bras, cut out soy, and started yoga. No meds. It’s 80% better. I’m not saying skip the doctor-but maybe try lifestyle first? 🌿✨
My sister had this after her baby passed away. The milk didn’t stop for 11 months. No tumor. No meds. Just grief. This article made me cry. Thank you for including that stress can do this. So many don’t understand.