A comprehensive guide comparing methotrexate with its main alternatives, covering mechanisms, side effects, costs, and how to choose the right therapy for rheumatoid arthritis.
Read MoreMethotrexate: Uses, Risks, and How to Manage Treatment
When working with Methotrexate, a folic‑acid antagonist used in cancer chemotherapy and autoimmune disease therapy. Also known as MTX, it works by blocking the enzymes that help cells copy DNA, which is why fast‑growing cells feel its effect first.
One of the biggest reasons doctors prescribe Methotrexate is for rheumatoid arthritis, a chronic joint inflammation that can erode bone and cartilage. The drug also tames psoriasis, a skin condition where immune cells overproduce skin cells, causing plaques. Because it suppresses the immune system, methotrexate is classified as an immunosuppressant, a medication that lowers the body’s defense against infections. These three entities create a clear chain: methotrexate treats rheumatoid arthritis and psoriasis, and its immunosuppressive action explains why patients need extra care to avoid infections like shingles.
Key considerations before starting methotrexate
Before the first dose, doctors run a baseline panel: liver enzymes, kidney function, and a blood count. This baseline is crucial because methotrexate can stress the liver and bone marrow. After that, patients usually get a low weekly dose, either as a pill or an injection, and the dose may be tweaked based on response and lab results. The weekly schedule is a hard rule—taking it daily can be toxic. Folic acid supplements are habitually added to blunt side effects; studies show that 1 mg of folic acid on the non‑dose day cuts nausea and mouth sores dramatically.
Side effects aren’t just stomach upset. Because methotrexate dampens immunity, viral infections can flare up. Shingles, for example, is more common in people on methotrexate, echoing concerns in the article “Shingles vs Flu”. Lung irritation, called pneumonitis, can also appear, especially in older patients or smokers. Regular check‑ups catch these problems early, and doctors may pause the drug if liver enzymes rise or breathing issues emerge. Interactions matter too—non‑steroidal anti‑inflammatories (NSAIDs) can raise methotrexate levels, and alcohol adds extra liver strain.
Managing methotrexate is a teamwork effort. Patients track doses, report any new rashes, shortness of breath, or unusual fatigue, and keep appointments for blood work every 4–8 weeks. Lifestyle tweaks—staying hydrated, avoiding high‑dose vitamin C around dosing, and limiting alcohol—help keep the drug’s safety profile in check. When everything aligns, methotrexate offers long‑term disease control without the need for steroids or more aggressive chemotherapy.
Below you’ll find a curated set of articles that dive deeper into the topics we just touched—how infections intersect with immunosuppressants, practical monitoring tips, and real‑world experiences from patients on methotrexate. Use them as a practical toolbox to stay informed and confident about your treatment plan.

Methotrexate vs Alternatives: Pros, Cons & How to Choose
Archive
Categories
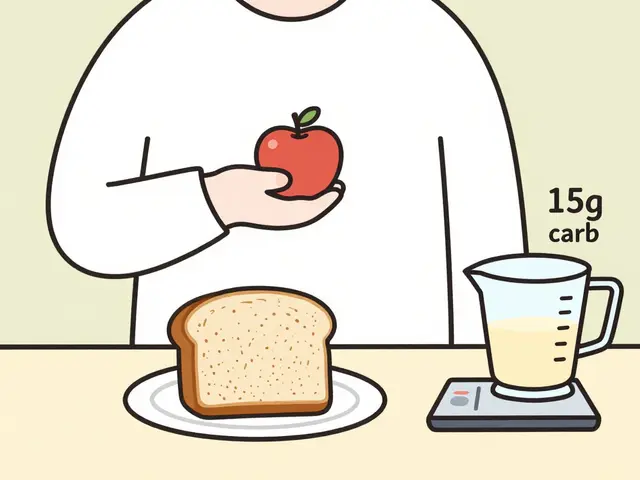
Carbohydrate Counting for Diabetes: A Complete Beginner's Guide
Learn how to count carbohydrates for diabetes management with this beginner-friendly guide. Understand portion sizes, insulin ratios, label reading, and real-world tips to control blood sugar without giving up your favorite foods.
Authorized Generics vs Traditional Generics: What You Need to Know
Authorized generics are the exact same drug as the brand-name version, just without the brand label. Traditional generics may have different inactive ingredients. Learn the key differences and how they affect your health and costs.
Patent Term Restoration (PTE): How It Extends Drug Patent Life
Patent Term Restoration (PTE) lets drug makers recover lost patent time due to FDA delays. Learn how it works, who qualifies, and why it's shaping drug prices and market access.

Digital Prescription Transfer: How to Move Your Scripts to Online Pharmacies
Learn how to transfer your prescriptions to online pharmacies with digital systems. Discover how DEA rules, transfer speeds, and insurance issues affect your switch-and how to avoid common mistakes.

Calcium-Fortified Juices and Medications: What You Need to Know About Binding and Absorption Issues
Calcium-fortified juices can severely reduce the absorption of key medications like antibiotics, thyroid hormones, and osteoporosis drugs. Learn which drugs are affected, how long to wait, and what to do to protect your treatment.