Rapid Drug Desensitization Simulator
Protocol Settings
Live Monitoring
Ready| Step | Concentration Factor | Cumulative Dose | Status |
|---|
Protocol Complete
Patient has reached the full therapeutic dose. Tolerance is established for this session. Maintenance phase begins.
You have a severe infection. The best antibiotic for you is penicillin. But your medical record says you are allergic to it. In the past, doctors might have given you a weaker alternative or added antihistamines to mask the reaction. Today, there is a more precise solution: drug desensitization. This process temporarily tricks your immune system into accepting a medication that would otherwise cause a dangerous reaction. It is not a cure for an allergy, but it is a bridge that allows life-saving treatments to continue.
This technique is standard care in hospitals like Brigham and Women's Hospital, where experts like Dr. Mariana Castells have refined these protocols over decades. If you or a loved one faces a situation where the best medicine is also the most risky, understanding how this works can reduce anxiety and help you advocate for safe treatment.
What Is Drug Desensitization?
Drug desensitization is a clinical procedure that induces temporary tolerance to a specific medication in patients who have previously experienced severe hypersensitivity reactions. Think of it as teaching your body to ignore a threat, but only for a short time. Your immune system has memory cells that recognize certain drugs as invaders. When you take the drug again, those cells trigger an attack-causing hives, swelling, or even anaphylaxis (a life-threatening drop in blood pressure).
Desensitization works by introducing tiny, sub-threshold amounts of the drug. These doses are too small to activate the mast cells and basophils that release histamine and other inflammatory chemicals. By slowly increasing the dose, usually doubling it every 15 to 30 minutes, the protocol saturates the receptors on these cells without triggering a full-scale response. Once the therapeutic dose is reached, the patient can complete their treatment course safely.
Crucially, this state of tolerance is temporary. If you stop the medication for even a few hours, your immune system "wakes up" again. You will need to go through the desensitization process for every single dose if the treatment spans multiple days. This is why it is typically done in a hospital setting with constant monitoring.
When Is Desensitization Used?
Doctors do not use this protocol for mild rashes or minor stomach upset. It is reserved for high-stakes scenarios where the benefits outweigh the risks. Here are the primary situations where desensitization becomes necessary:
- No Alternative Exists: For some infections, particularly resistant bacteria, penicillin or vancomycin may be the only drugs that work. Substituting with a less effective antibiotic could lead to treatment failure or sepsis.
- Superior Efficacy: In oncology, certain chemotherapy drugs (like taxanes) or targeted therapies (monoclonal antibodies) are significantly more effective than alternatives. If a patient develops hypersensitivity, switching drugs could compromise cancer survival rates.
- Autoimmune Conditions: Patients with rheumatoid arthritis or asthma may rely on aspirin or NSAIDs. If they develop sensitivity, desensitization allows them to maintain pain control and inflammation management without switching to less potent options.
- Critical Care: In emergency settings, such as treating neurosyphilis or Lyme carditis, the specific drug required is non-negotiable for preventing permanent organ damage.
According to guidelines from the American Academy of Allergy, Asthma & Immunology (AAAAI), desensitization is strongly recommended (Grade 1A) for IgE-mediated immediate hypersensitivity reactions to essential medications. However, it is strictly contraindicated for severe delayed skin reactions like Stevens-Johnson syndrome or toxic epidermal necrolysis. In those cases, the risk of fatal skin detachment is too high, and alternative treatments must be found.
Rapid vs. Slow Desensitization Protocols
Not all allergies react at the same speed. Therefore, the protocol used depends on the type of immune response involved. There are two main categories:
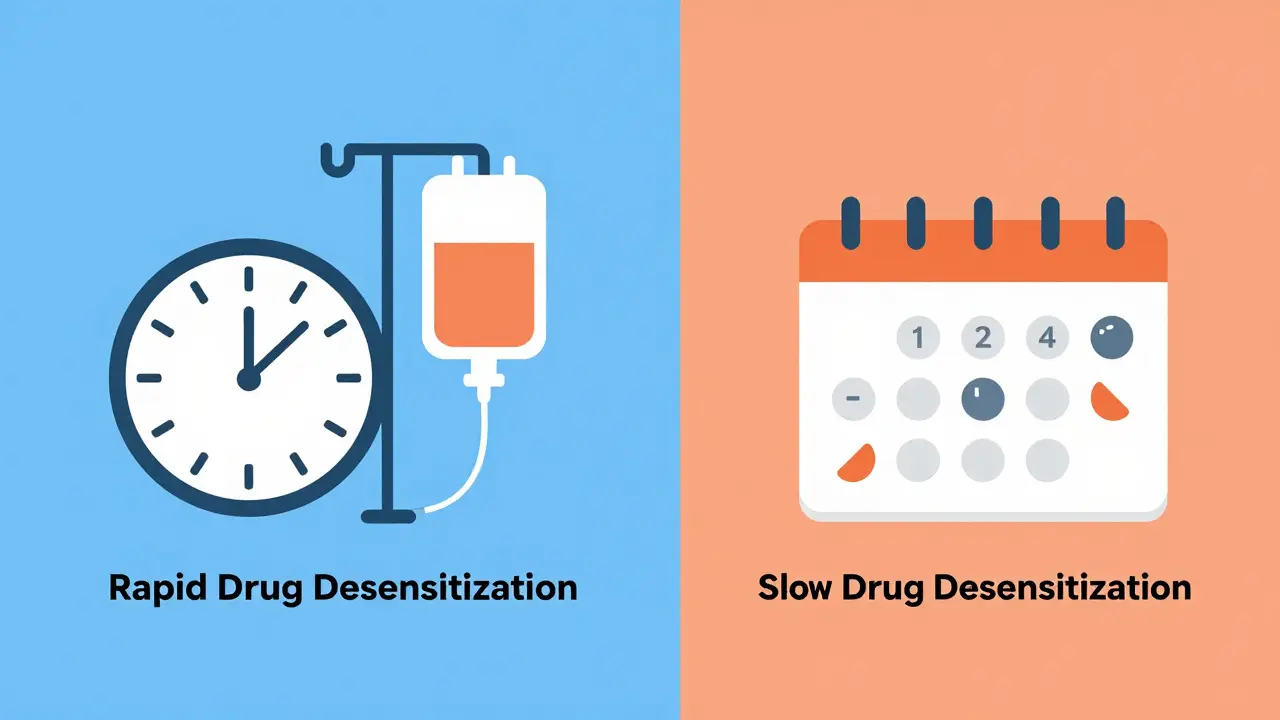
| Feature | Rapid Drug Desensitization (RDD) | Slow Drug Desensitization (SDD) |
|---|---|---|
| Type of Reaction | Immediate (IgE-mediated, occurs within minutes to hours) | Delayed (T-cell mediated, occurs days later) |
| Common Drugs | Antibiotics (Penicillin, Vancomycin), Chemotherapy (Taxanes) | NSAIDs, Aspirin, Allopurinol, Sulfonamides |
| Dosing Interval | Every 15-30 minutes | Every several hours to days |
| Duration | 4-6 hours per session | Several days to weeks |
| Route | Intravenous (IV) or Oral | Primarily Oral |
| Success Rate | 95-100% | Variable (75% in early trials) |
Rapid Drug Desensitization (RDD) is the most common approach. It follows a standardized geometric progression. For example, a typical IV protocol might start with a dose that is 1/10,000th of the target therapeutic dose. Over 12 steps, the concentration doubles each time. By step 12, the patient receives the full daily requirement. This entire process takes about 4 to 6 hours. During this time, nurses monitor blood pressure, oxygen levels, and heart rate continuously.
Slow Drug Desensitization (SDD) is used for delayed reactions, which involve T-cells rather than IgE antibodies. Because the reaction takes longer to manifest, the dosing intervals are much wider. An aspirin desensitization protocol, for instance, might involve taking tiny amounts of aspirin orally every few hours over the course of two to three days. There is less consensus on the exact steps for SDD compared to RDD, so protocols can vary between institutions.
The Procedure: What to Expect
If you are scheduled for desensitization, preparation is key. You will likely be admitted to a hospital or a specialized day unit. Here is what the process looks like from start to finish:
- Pre-Assessment: An allergist or immunologist reviews your history. They confirm that the reaction was truly an allergy and not a side effect (like nausea). They also check for contraindications, such as uncontrolled asthma or recent anaphylaxis.
- Setup: You will be placed in a room equipped with resuscitation gear. This includes epinephrine, antihistamines, corticosteroids, and airway management tools. Continuous cardiac and pulse oximetry monitoring begins.
- Dilution Preparation: Pharmacists prepare a series of diluted solutions. Accuracy is critical; errors here can lead to adverse events. Standardized dilution kits help reduce preparation mistakes by 75%.
- Administration: The first micro-dose is given. You wait 15 to 30 minutes. If no reaction occurs, the next double dose is administered. This repeats until the full dose is reached.
- Maintenance: Once the full dose is achieved, you receive the remainder of your treatment for that day. If the medication is needed for multiple days, you must return for desensitization before each subsequent dose.
During the process, mild symptoms like itching or flushing can occur in about 8% of cases. These are usually managed with antihistamines without stopping the protocol. Severe reactions (anaphylaxis) are rare (<2%) when performed by trained specialists in appropriate facilities.
Why Not Just Use Antihistamines?
A common question is why doctors don't just pre-medicate with Benadryl (diphenhydramine) or steroids. While premedication helps with infusion reactions (non-allergic side effects), it does not prevent true IgE-mediated allergic reactions. Studies show that premedication fails in up to 40% of cases involving hypersensitivity. Desensitization, by contrast, has a success rate of 98-100% for immediate reactions. It addresses the root mechanism of the allergy rather than just masking the symptoms.
Furthermore, substitution often leads to worse outcomes. For example, substituting penicillin with clindamycin increases the risk of C. difficile infection. Substituting with broader-spectrum antibiotics contributes to antimicrobial resistance. Desensitization allows the use of narrow-spectrum, highly effective drugs, preserving the efficacy of our antibiotic arsenal.

Risks and Limitations
While safe in expert hands, desensitization is not without risks. The biggest danger is performing the procedure in an unprepared setting. Data shows that complication rates are three times higher in community hospitals where non-specialists attempt desensitization without proper monitoring equipment. Always seek care at a center with board-certified allergists and immunologists.
Another limitation is resource intensity. A single desensitization session requires approximately 4.2 nursing hours and 1.8 physician hours. This makes it expensive and logistically challenging. Insurance coverage varies, with some payers covering only 60% of the actual costs, creating financial barriers for smaller institutions.
Finally, remember that desensitization is temporary. If you miss a dose by more than a few hours, the tolerance breaks down. You cannot simply "take the pill at home" after being desensitized in the hospital. This requires strict adherence to the schedule.
Future Directions in Desensitization
The field is evolving rapidly. Researchers are working on biomarker-guided desensitization. Tests like basophil activation tests can now predict success with 89% accuracy, helping doctors decide who is a good candidate before starting the protocol. Additionally, home-based protocols are in phase 2 trials, showing 92% success rates for stable patients. This could eventually allow patients to undergo desensitization in the comfort of their homes, reducing hospital stays and costs.
As antibiotic resistance rises-with the CDC reporting 35,000 annual deaths in the US from resistant infections-the ability to use last-resort antibiotics via desensitization will become increasingly vital. Within five years, genetic and immunologic profiling may determine exactly which protocol will succeed for each individual patient, moving us toward precision allergy care.
Is drug desensitization permanent?
No, drug desensitization induces only temporary tolerance. The immune system returns to its sensitized state once the medication is stopped. If the drug is needed again after a break (usually more than 2-4 half-lives of the drug), the desensitization protocol must be repeated from the beginning.
Can I be desensitized to any medication?
It depends on the type of reaction. Desensitization is highly effective for immediate (IgE-mediated) reactions to antibiotics, chemotherapy, and NSAIDs. However, it is generally contraindicated for severe delayed cutaneous reactions like Stevens-Johnson syndrome or toxic epidermal necrolysis due to the high risk of life-threatening complications.
How long does the desensitization process take?
Rapid Drug Desensitization (RDD) typically takes 4 to 6 hours for intravenous medications. Slow Drug Desensitization (SDD) for oral medications like aspirin can take several days, with doses spaced hours apart. Each subsequent dose of the medication during the treatment course may require a new desensitization session.
What are the risks of drug desensitization?
The primary risk is an allergic reaction, ranging from mild itching to severe anaphylaxis. However, when performed by trained specialists in a monitored setting, severe reactions occur in less than 2% of cases. The procedure requires immediate access to emergency medications like epinephrine and airway support.
Do I need to stay in the hospital for desensitization?
Yes, typically. Because of the risk of anaphylaxis, desensitization should be performed in a hospital or specialized clinic with continuous monitoring capabilities. Home-based protocols are currently experimental and not yet standard care, though trials show promise for stable patients.