When you start a new medication, you expect it to help with your condition. But what if it also makes you constantly hungry-or suddenly lose interest in food? Appetite changes from medication are more common than most people realize. They don’t just affect your waistline; they can mess with your energy, mood, sleep, and even how well your treatment works. The truth is, this isn’t a personal failing. It’s a biological response built into how some drugs interact with your brain and body.
Why Your Appetite Changes When You Take Medicine
Your appetite isn’t controlled by willpower. It’s ruled by chemicals in your brain-serotonin, dopamine, ghrelin, and histamine-that tell you when you’re hungry or full. Many medications accidentally bump these signals out of balance.
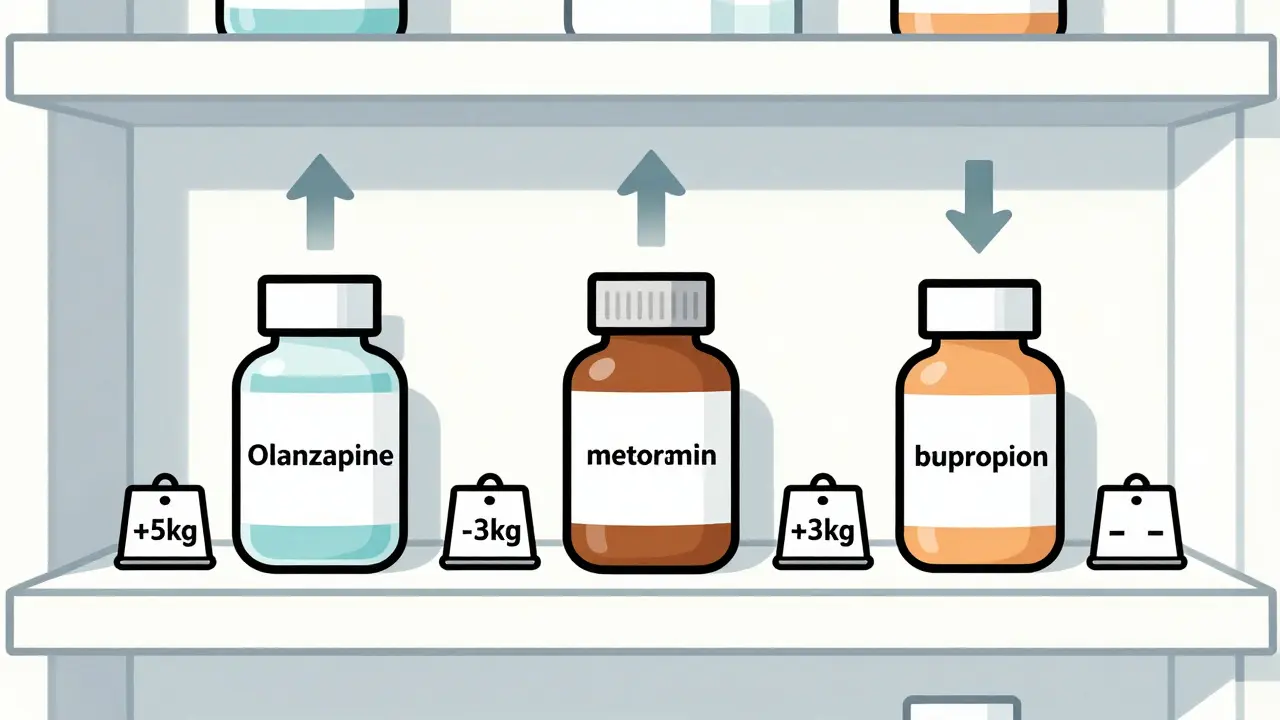
Take antipsychotics like olanzapine is a second-generation antipsychotic that increases ghrelin, the "hunger hormone," by 15-20% within weeks. That’s why some people gain 5-10 pounds in just 10 weeks. It’s not laziness. It’s pharmacology.
Antidepressants work differently. Short-term use of drugs like sertraline is an SSRI that may reduce appetite by boosting serotonin, which increases feelings of fullness can make you eat less. But after a year? That same serotonin system starts to adapt. Your brain downregulates receptors, and suddenly you’re craving carbs. Studies show 35% of long-term users develop intense cravings for bread, pasta, or sweets.
Then there are stimulants like amphetamines. These drugs shut down hunger by flooding your system with norepinephrine and dopamine. People on ADHD meds often report eating one meal a day. That’s not normal-it’s a side effect. Research shows they consume 300-500 fewer calories daily than before starting treatment.
Even diabetes meds aren’t immune. insulin helps cells absorb glucose, but it also signals fat storage. Many patients gain 2-4 kg in six months. Meanwhile, metformin works differently-it improves insulin sensitivity and reduces liver glucose output, which often leads to modest weight loss. So two drugs for the same condition can have opposite effects on your appetite.
Which Medications Are Most Likely to Change Your Appetite?
Not all drugs affect appetite the same way. Some are notorious. Others rarely cause issues. Here’s what the data shows:
| Medication Class | Examples | Appetite Effect | Average Weight Change (6 Months) |
|---|---|---|---|
| Antipsychotics | Olanzapine, Risperidone, Quetiapine | Strong increase | +5 to +10 kg |
| Antidepressants | Mirtazapine, Amitriptyline, Paroxetine | Increase | +2 to +5 kg |
| Antidepressants | Bupropion, Vortioxetine | Decrease or neutral | −1 to +0.5 kg |
| Diabetes Meds | Insulin, Sulfonylureas | Increase | +2 to +4 kg |
| Diabetes Meds | Metformin | Decrease | −2 to −3 kg |
| Mood Stabilizers | Lithium | Increase | +3 to +5 kg |
| Antihistamines | Diphenhydramine, Hydroxyzine | Mild increase | +1 to +2 kg |
| Appetite Suppressants | Topiramate, Liraglutide | Strong decrease | −3 to −5 kg |
Notice something? Mirtazapine is one of the worst offenders among antidepressants. About 40% of users gain over 7% of their body weight in six months. Meanwhile, bupropion is one of the few antidepressants that may actually help you lose weight. If weight is a concern, this isn’t just a side note-it’s a critical choice.
How to Manage Increased Appetite
If your medication is making you hungry all the time, don’t just try to "eat less." That rarely works long-term. You need to rewire your environment and habits.
- Fill up on fiber. Whole grains, beans, lentils, and vegetables take longer to digest. Studies show they extend satiety by 20-30 minutes per meal. Swap white bread for sourdough. Pick brown rice over white.
- Plan protein snacks. Eat 15-20 grams of protein every 3-4 hours. That’s a hard-boiled egg, a small cup of Greek yogurt, or a handful of almonds. Protein stabilizes blood sugar and reduces hunger spikes by 40%.
- Prep meals twice a week. People who meal prep consume 200 fewer calories daily than those who eat spontaneously. It’s not about willpower-it’s about removing temptation.
- Drink water before meals. A 2022 study found that drinking two glasses of water 30 minutes before eating reduced calorie intake by 13% on average. Your brain confuses thirst for hunger.
- Remove high-calorie snacks. If chips, cookies, or candy aren’t in the house, you can’t grab them mindlessly. Behavioral studies show this cuts impulsive eating by 35%.
And don’t underestimate movement. Resistance training-even just two 30-minute sessions a week-builds muscle. Each 1% increase in muscle mass raises your resting metabolism by 50-100 calories per day. That’s like burning an extra apple every 24 hours.
How to Manage Decreased Appetite
Loss of appetite is just as dangerous-if not more so. If you’re not eating enough, you risk muscle loss, fatigue, and weakened immunity.
- Eat smaller, more frequent meals. Instead of three big meals, try five small ones. Your body can handle more food spread out.
- Boost calorie density. Add nut butter to toast, olive oil to pasta, or cheese to eggs. You don’t need to eat more volume-you need more energy per bite.
- Use flavor. Loss of appetite often comes with reduced taste sensitivity. Spices, herbs, citrus, and umami-rich foods (like mushrooms or soy sauce) can make food more appealing.
- Don’t skip breakfast. Even if you’re not hungry, eating something within an hour of waking helps reset your hunger rhythm.
- Try liquid calories. Smoothies with protein powder, milk, banana, and peanut butter can be easier to consume than solid food when appetite is low.
When to Talk to Your Doctor
Never stop or switch meds on your own. Abruptly quitting antipsychotics, antidepressants, or seizure meds can cause seizures, psychosis, or severe withdrawal. But you can have a conversation with your provider.
Here’s what to say:
- "I’ve gained X pounds since starting Y medication. Is there a weight-neutral alternative?"
- "I’ve lost my appetite and am losing muscle. Can we adjust the dose?"
- "I’m struggling with cravings. Is there a medication that helps with both my condition and weight?"
Doctors are now trained to ask about weight changes. In 2022, 65% of primary care physicians routinely screened for medication-induced weight gain-up from 35% in 2015. You’re not being dramatic. You’re being smart.
Some newer drugs are designed to avoid this problem. Vortioxetine causes only 0.5 kg of weight gain over six months, compared to 2.5 kg for older SSRIs. Auvelity (dextromethorphan/bupropion) shows just 0.7% average weight gain in trials. And KarXT (xanomeline-trospium), a new antipsychotic in phase 3 trials, caused only 0.4 kg of weight gain versus 3.2 kg for olanzapine. These aren’t sci-fi-they’re real, approved, and available now.
What Works Best: Behavior + Medication
The best outcomes come from combining two things: smart habits and smart meds.
Studies show that if you start behavioral changes at the same time you begin a new medication, you cut weight gain in half. That’s not magic. It’s science. A 2022 study from the University of Toronto found that patients who followed a structured plan-meal timing, protein snacks, weekly weigh-ins, and resistance training-gained 50% less weight than those who waited until they gained 10 pounds.
And if you’re on a medication that causes weight gain, ask if adding topiramate can help counteract it. It’s not just for seizures. It’s a proven appetite suppressant. In 60% of users, it leads to 3-5 kg of weight loss over six months. Used carefully, it can be a tool to balance out side effects.
Final Thoughts
Appetite changes from medication aren’t your fault. They’re a biological side effect, often predictable, and always manageable. You don’t have to choose between treating your condition and staying healthy. The tools exist. The knowledge is out there. The key is to speak up early, track changes, and work with your care team-not against them.
Weight gain or loss isn’t just about food. It’s about how your body responds to chemistry you didn’t choose. But you still have control-over your habits, your questions, and your next steps.
Can medication-induced appetite changes be reversed?
Yes, in many cases. If the medication is stopped or switched, appetite often returns to normal over weeks to months. But if weight gain has led to insulin resistance or metabolic changes, those may need separate management through diet, exercise, or medications like metformin. Early intervention is key-waiting until you’ve gained 20 pounds makes reversal harder.
Why do some people gain weight on antidepressants while others lose it?
It depends on the drug and your biology. SSRIs like sertraline often reduce appetite early on, but long-term use can trigger cravings. Mirtazapine increases appetite by blocking histamine receptors. Bupropion suppresses appetite by affecting dopamine and norepinephrine. Genetics also play a role-some people have receptors that respond more strongly to certain chemicals. That’s why one person gains 15 pounds on paroxetine and another loses 5.
Is it safe to take weight-loss drugs with psychiatric medications?
Sometimes, but only under medical supervision. Topiramate and bupropion are often used together for this purpose. However, combining appetite suppressants with stimulants or certain antidepressants can raise blood pressure or trigger serotonin syndrome. Always consult your prescriber before adding any new medication-even over-the-counter ones.
How long does it take for appetite to return to normal after stopping a medication?
It varies. For most people, hunger cues return within 2-6 weeks after stopping a drug. But if the medication caused long-term metabolic changes-like insulin resistance-it can take months. Blood sugar levels, leptin, and ghrelin need time to rebalance. Don’t expect instant results. Patience and consistent habits matter more than speed.
Can lifestyle changes alone fix medication-induced weight gain?
Lifestyle changes help, but they rarely fully offset strong biological effects. Someone on olanzapine might eat perfectly and still gain weight because the drug is overriding their natural hunger signals. That’s why the best approach combines behavior changes with medication review. You can’t out-exercise a pharmacological side effect.




11 Comments
So let me get this straight-you’re telling me my 12-pound gain on olanzapine isn’t because I’m lazy, but because my brain got hacked by a pharmaceutical company’s chemistry experiment? Finally. Someone said it. I’ve been told to "just eat less" like I’m some kind of moral failure. Newsflash: I’m not choosing to crave pizza at 2 a.m. My dopamine receptors are on a sugar bender, and I’m just along for the ride.
And don’t even get me started on how no one talks about the shame spiral. You gain weight, you feel like crap, you stop exercising, you feel worse, you eat more. It’s a loop designed by someone who never had to live with this shit. I’m not here to be inspirational. I’m here to say: this isn’t your fault. It’s a damn side effect.
Pharmaceutical industry manipulation. Always. They design drugs to create dependency-weight gain means more meds, more doctor visits, more profits. It’s not an accident. It’s business.
GHRELIN modulation via CB1 agonism is a well-documented off-target effect of second-gen antipsychotics. Olanzapine’s affinity for H1 and M3 receptors further exacerbates metabolic dysregulation. Stop pathologizing hunger-it’s pharmacokinetics.
Thank you for this thoughtful and scientifically grounded post. As someone who has seen many patients struggle with these exact issues, I am deeply moved by how clearly you have explained the biological mechanisms behind appetite changes. Many in my community are unaware that this is not a personal failing, but a physiological response. Your work here is truly helpful.
wait so metformin makes you lose weight? i thought it was just for diabetics?? i’ve been taking it for my acne and i lost 15lbs?? is this legit??
I just want to say… you’re not alone. I was on mirtazapine for two years. Gained 20 pounds. Felt like a stranger in my own body. I cried every time I stepped on the scale. But then I started meal prepping, adding protein snacks, and drinking water before meals. Not because I wanted to lose weight-but because I wanted to feel like myself again.
It didn’t fix everything. But it gave me back some control. And that matters more than the number on the scale.
YES THIS!! I’m on vyvanse and barely eat all day. Then at 10pm I’m eating an entire pizza like a zombie 😅
Drink water before meals? I didn’t even know that was a thing. Gonna try it. Thanks for sharing!!
Your comprehensive breakdown of medication-induced appetite changes is both clinically accurate and deeply human. The distinction between short-term and long-term pharmacological effects on serotonin receptors is particularly insightful. I would encourage all clinicians to reference this as a patient education tool. The behavioral interventions you outline are evidence-based and accessible, making them ideal for primary care integration.
My sister’s on lithium and gained 30 lbs. She felt like a failure. I showed her this post. She cried. Then she called her doctor. We’re all just trying to survive. Thanks for making it okay to talk about this.
There is no such thing as "medication-induced" weight gain. It is always behavioral noncompliance masked by pharmacological rhetoric. The data you cite is correlational, not causal. You are reinforcing medical victimhood culture. Real solutions require discipline, not dietary hacks.
Oh wow. You’re the same person who told me to "just get up and move" when I was in a depressive episode on antipsychotics? You don’t get to act like you’re above this. You’re not a doctor. You’re not even a patient. You’re just another guy with a keyboard and zero empathy.
And yeah, I’m still here. Still eating. Still surviving. And I’m not apologizing for it.