For those dealing with this, the goal is three-fold: stop the active leak, keep it from happening again, and manage the pressure that caused it in the first place. Depending on the severity, this usually involves a combination of a procedure called banding, long-term medication, and in some high-risk cases, a surgical shunt.
Stopping the Bleed: How Endoscopic Band Ligation Works
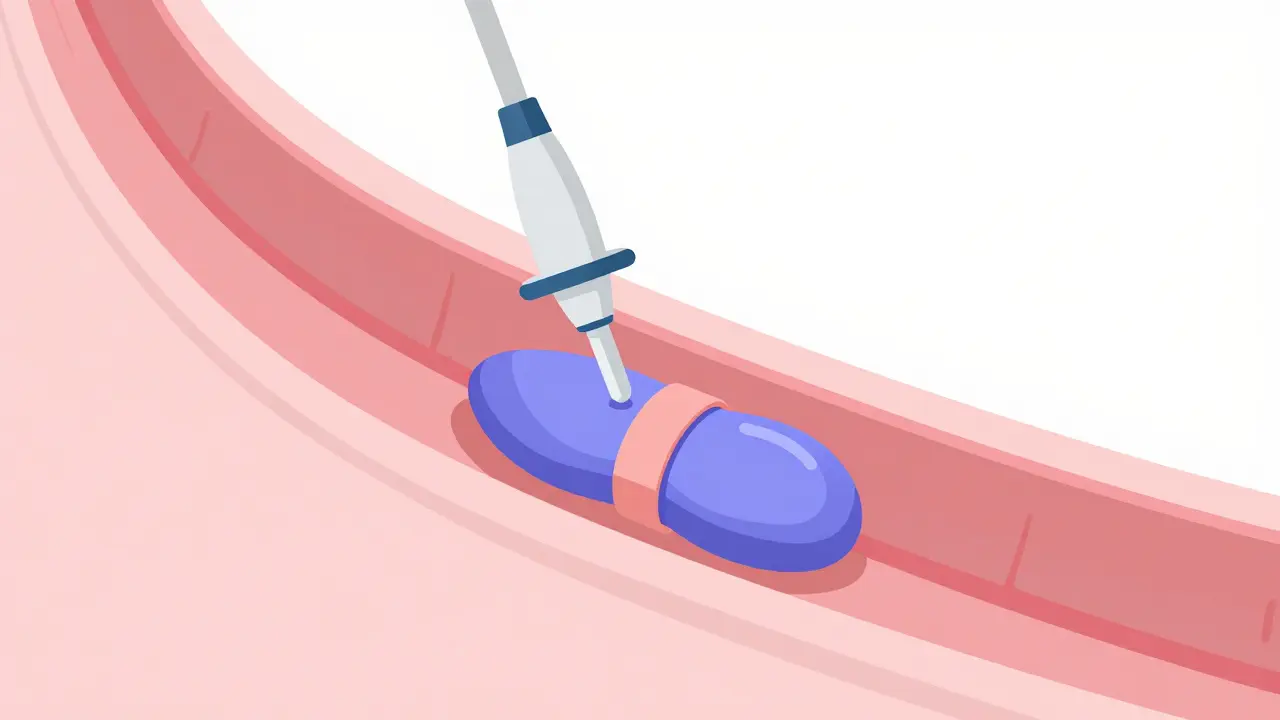
When a patient arrives at the hospital with active bleeding, the clock is ticking. Guidelines from the AASLD suggest that the procedure to stop the bleed should happen within 12 hours. The current gold standard is Endoscopic Band Ligation is a procedure where a gastroenterologist uses an endoscope to place small rubber bands around the bleeding varices. Also known as EBL, this technique effectively cuts off blood flow to the varix, causing it to clot and eventually wither away.
It is far more effective than the older method of sclerotherapy (injecting chemicals to shrink the veins), which carried a higher risk of scarring the esophagus. Modern tools, like the Boston Scientific Six-Shot Banding System, allow doctors to deploy multiple bands quickly, reducing the time a patient spends under sedation. However, it's rarely a one-and-done deal. Most people need 3 to 4 sessions, spaced about a week or two apart, to completely clear the varices from their system.
While the success rate for stopping initial bleeding is impressive-around 90-95%-it isn't without downsides. Some patients report significant throat pain and difficulty swallowing for a couple of weeks after the procedure. Despite the discomfort, the alternative is far worse; the immediate control of bleeding is what saves lives in the ER.
Long-Term Pressure Control with Beta-Blockers
Stopping the bleed is the immediate fix, but you have to address the "pressure" problem to prevent a recurrence. This is where Non-selective Beta-Blockers is a class of medications that reduce the heart rate and constrict blood flow to the organs in the abdomen to lower portal vein pressure. Commonly referred to as NSBBs, they act as a chemical shield for the liver.
There are two heavy hitters in this category: Propranolol and Carvedilol. Propranolol is the traditional choice, often starting at a low dose of 20mg twice daily and scaling up. However, Carvedilol is increasingly preferred because it typically reduces portal pressure more effectively-by about 22% compared to 15% for Propranolol. By bringing the pressure down, the risk of a vein bursting is cut roughly in half.
The catch? These drugs can be tough to tolerate. Many patients experience extreme fatigue, dizziness, or a slow heart rate. In some cases, up to 30% of people struggle to reach the full therapeutic dose because the side effects are too intense. If you feel like you're constantly exhausted on these meds, it's a common side effect and something to discuss with your doctor for dose adjustment.
| Treatment | Primary Goal | Key Advantage | Main Drawback |
|---|---|---|---|
| Banding (EBL) | Acute Hemostasis | Fast, high success rate (90%+) | Requires multiple sessions; throat pain |
| Beta-Blockers (NSBBs) | Prevention/Pressure Control | Low cost, reduces rebleeding by 50% | Fatigue, dizziness, low heart rate |
| TIPS Shunt | High-Risk Pressure Relief | Superior 1-year survival for Child-Pugh B/C | Risk of hepatic encephalopathy |
When Banding Isn't Enough: The Role of TIPS
Some patients are too sick for medications or too high-risk for simple banding. For them, a more aggressive approach is needed: Transjugular Intrahepatic Portosystemic Shunt is a procedure that creates a man-made channel (shunt) in the liver to reroute blood flow and bypass the blockage. Commonly called TIPS, it is the heavy-duty option for portal hypertension.
TIPS can be a lifesaver for those with severe liver failure (Child-Pugh B or C) who are actively bleeding. Research shows that high-risk patients receiving a TIPS procedure have a significantly higher one-year survival rate (86%) compared to those receiving standard care (61%). It basically solves the plumbing problem by creating a detour for the blood.
The trade-off is the risk of hepatic encephalopathy-a condition where toxins that the liver normally filters out instead go straight to the brain, causing confusion or sleep disturbances. About 30% of TIPS patients deal with this, compared to only 10% of those on standard care. It's a balancing act between preventing a fatal bleed and managing mental clarity.
Preventing the First Bleed: Primary Prophylaxis
The best-case scenario is preventing the first bleed entirely. This is called primary prophylaxis. Doctors use a combination of screening-usually via endoscopy-and preventative treatment. If a patient is found to have "high-risk" varices (those that are large or already showing signs of imminent rupture), the strategy is usually a choice between NSBBs or EBL.
Recent data suggests that Carvedilol might be just as effective as banding for primary prevention, which is great news for patients who want to avoid repeated hospital visits for endoscopic procedures. The trend is moving toward a "patient-centered" approach: if you can tolerate the meds, take them; if you can't, go for the bands.
Prevention also means managing the underlying cause. Whether it's treating Hepatitis C with modern antivirals or maintaining strict alcohol abstinence, reducing the damage to the liver is the only way to truly lower the portal pressure permanently.
Common Pitfalls and Patient Realities
In a perfect world, every patient gets an endoscopy within 12 hours and hits their target beta-blocker dose within three months. In reality, the system is clunky. Only about 68% of patients actually receive the timely endoscopy recommended by guidelines. Furthermore, many people stop taking their beta-blockers because they feel "too tired to function," not realizing that stopping the drug significantly increases their risk of a catastrophic bleed.
There's also a psychological toll. Imagine having to go back to a clinic every two weeks for a procedure that makes it hard to swallow. The mental exhaustion of chronic liver disease, combined with the fear of a sudden bleed, is something that often goes unaddressed. Support groups and nurse navigators are essential here to help patients stay adherent to their treatment plans.
What is the difference between primary and secondary prevention?
Primary prevention is for people who have varices but have never bled; the goal is to stop the first bleed from ever happening. Secondary prevention is for people who have already had a variceal bleed; the goal is to prevent a second episode, which is much more dangerous. Secondary prevention usually requires a more aggressive combination of both banding and beta-blockers.
Can I stop taking beta-blockers if I feel too tired?
You should never stop these medications without consulting your doctor. While fatigue is a common and frustrating side effect, stopping the medication can lead to a rapid increase in portal pressure, potentially triggering a life-threatening bleed. Your doctor may be able to switch you from Propranolol to Carvedilol or adjust your dose to make it more tolerable.
Is banding a permanent cure for varices?
No, banding is not a cure for the underlying liver disease. It treats the symptom (the swollen veins) by tying them off. Because the portal hypertension (the high pressure) is still there, new varices can form over time. This is why regular follow-up endoscopies and long-term medication are necessary.
How soon after a bleed should I have a follow-up?
Initial hemostasis should happen within 12 hours of presentation. After the first banding session, subsequent sessions are typically scheduled every 1 to 2 weeks until the varices are completely eradicated. Long-term monitoring varies, but quarterly or bi-annual check-ups are common depending on the risk level.
What are the signs that a varix might be bleeding?
The most obvious sign is vomiting blood (hematemesis) or passing black, tarry stools (melena). Other signs include sudden dizziness, fainting, or a rapid heart rate. This is a medical emergency-if you experience these symptoms, go to the ER immediately.
Next Steps and Troubleshooting
If you or a loved one has been diagnosed with liver cirrhosis and varices, the first priority is establishing a relationship with a hepatologist or gastroenterologist who specializes in portal hypertension.
- For those starting Beta-Blockers: Keep a daily log of your heart rate and blood pressure. If your heart rate drops below 60 bpm or you feel faint, contact your clinic immediately for a dose adjustment.
- For those undergoing Banding: Use soft foods and avoid scratchy or hard foods for the first few days after the procedure to minimize irritation in the esophagus.
- For those with severe failure: Ask your medical team about your Child-Pugh score. If you are in category B or C, ask if an early TIPS procedure is a safer option than medication alone.


13 Comments
Carvedilol seems like a much better bet than Propranolol if the pressure reduction is actually 22%. It's interesting that the medical community is shifting toward a more patient-centered approach for primary prevention.
why do people even struggle with the meds just take them and stop complaining about being tired lol some people just have zero willpower
Easy there. Fatigue from beta-blockers isn't just 'being tired', it's a physiological drop in heart rate and blood pressure. You can't just 'willpower' your way out of a slow heart rate.
It is imperative to note that the Child-Pugh score is a critical determinant in the decision-making process for a TIPS procedure. For patients in category C, the risk-benefit ratio heavily favors the shunt due to the catastrophic nature of recurrent bleeding in decompensated cirrhosis. Furthermore, the management of hepatic encephalopathy post-TIPS often requires a strict regimen of lactulose and rifampin to maintain cognitive function, which is a significant lifestyle adjustment for the patient. Proper nutritional support, specifically a high-protein diet tailored to liver failure, is also essential to mitigate the risk of muscle wasting and further decline in liver function. The synergy between pharmacological pressure control and mechanical intervention is what truly optimizes survival rates in these complex cases.
I appreciate the detailed breakdown of the TIPS procedure. It's a heavy-duty option, but for some, it's the only way to keep the pressure in check.
Honestly, only some of us truly understand the nuance of portal hypertension. It's just such a tragedy when people don't follow the 12-hour window for endoscopy-I mean, it's basic medical literacy at this point, really. It's simply embarrassing that the system is this clunky in a developed country.
The inefficiency of the current healthcare delivery system is absolutely abhorrent! Only 68% of patients receiving timely endoscopy is not a statistic; it is a systemic failure of the highest order! It is a disgraceful display of negligence that patients are left to perish due to administrative incompetence!
Life is a journey and we must stay strong! :) Every small step in treatment is a win for the soul. Keep smiling and keep fighting! 🌟
Oh my goodness, the thought of vomiting blood is just too terrifing to think about!! I hope evryone is getting their checkups on time because this sounds like a total nightmare of a situation!!
The fragility of the human vessel... it is truly a testament to how a single blockage can redefine a whole existence... the pressure builds... the walls thin... it is a poetic yet terrifying spiral.
Totally agree that the psychological part is ignored. Living with the fear of a sudden bleed is a huge mental burden that most people don't get.
The information provided regarding the pharmacological options is most comprehensive.
It's just wild how a rubber band is the go-to fix for something this serious. Nature is brutal, but the fixes we come up with are even wilder!