Discover how clavulanic acid boosts bronchitis treatment, its mechanism, dosage, safety tips, and why it outperforms amoxicillin alone.
Read MoreAntibiotic for Bronchitis: What You Need to Know
When dealing with antibiotic for bronchitis, a medication prescribed to clear bacterial infection in the bronchial tubes. Also known as bronchitis antibiotics, it plays a key role in stopping the infection before it spreads to the lungs.
Bronchitis is the inflammation of the large airways that carry air to the lungs. It can be triggered by viruses, bacteria, or irritants like smoke. Most cases start as viral, so an antibiotic for bronchitis is only useful when a bacterial cause is confirmed or highly suspected. Typical signs that point to a bacterial infection include a high fever lasting more than three days, thick yellow‑green sputum, and worsening shortness of breath after the initial viral phase.
Choosing the Right Antibiotic
Doctors often start with a narrow‑spectrum doxycycline for healthy adults because it covers the most common bacterial culprits like Haemophilus influenzae and atypical walkers such as Mycoplasma pneumoniae. If a patient is allergic to tetracyclines or has specific risk factors, amoxicillin (sometimes combined with a beta‑lactamase inhibitor) becomes the go‑to choice. Macrolides like azithromycin are saved for those with penicillin allergies or when atypical pathogens dominate the picture.
Choosing an antibiotic isn’t random; it follows the principle that antibiotic for bronchitis treats bacterial infection. However, overuse fuels antibiotic resistance, making future infections harder to cure. Guidelines now recommend a sputum culture or rapid antigen test whenever possible, especially in patients with COPD, recent hospitalization, or exposure to healthcare settings.
Dosage and duration matter, too. A typical doxycycline course runs 100 mg twice daily for five to seven days, while amoxicillin is usually 500 mg three times a day for the same period. Shorter courses (three to five days) have shown equal effectiveness for uncomplicated cases and reduce side‑effects like diarrhea and yeast infections. Children under eight, pregnant women, and people with liver disease need dose adjustments or alternative agents.
Special populations shift the treatment picture. Smokers and those with chronic obstructive pulmonary disease often harbor resistant strains, so a fluoroquinolone might be added only after culture results confirm the need. Immunocompromised patients, such as those on chemotherapy, may require broader‑spectrum agents and longer treatment to prevent complications like bronchiectasis.
Practical tips help patients get the most out of their therapy: take the antibiotic with a full glass of water, avoid dairy if the drug is a tetracycline, and finish the entire course even if you feel better. Missing doses can let bacteria bounce back, leading to relapse and resistance. If side‑effects become severe—persistent nausea, rash, or severe diarrhea—contact your healthcare provider right away.
Below you’ll find a curated collection of articles that dive deeper into specific antibiotics, compare treatment guidelines, and offer step‑by‑step advice for buying safe generic options online. Whether you’re looking for dosing charts, side‑effect management, or the latest research on resistance patterns, the posts ahead give you the tools to make an informed choice.

Clavulanic Acid: How It Transforms Bronchitis Treatment
Archive
Categories

Managing Healthcare Resources During Novel Influenza Outbreaks
Learn how novel influenza strains strain hospitals and discover practical steps to manage beds, staff, PPE, and vaccines during outbreaks.
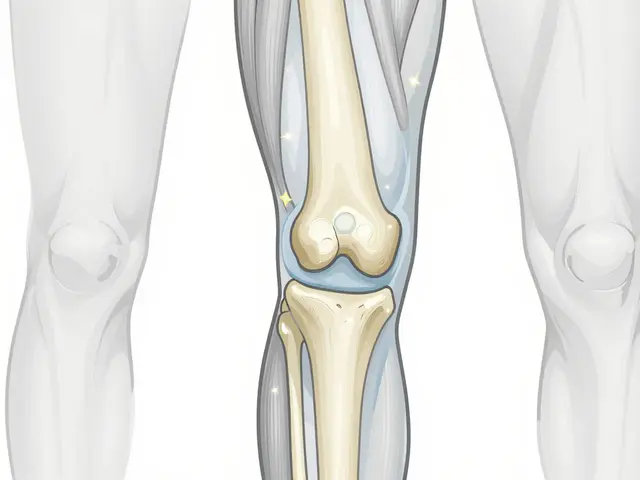
Osteoarthritis: How Joint Degeneration Works and What Actually Helps with Pain
Osteoarthritis isn't just aging-it's a treatable joint disease. Learn how cartilage breaks down, why movement helps more than rest, and the four science-backed strategies that actually reduce pain and improve mobility.
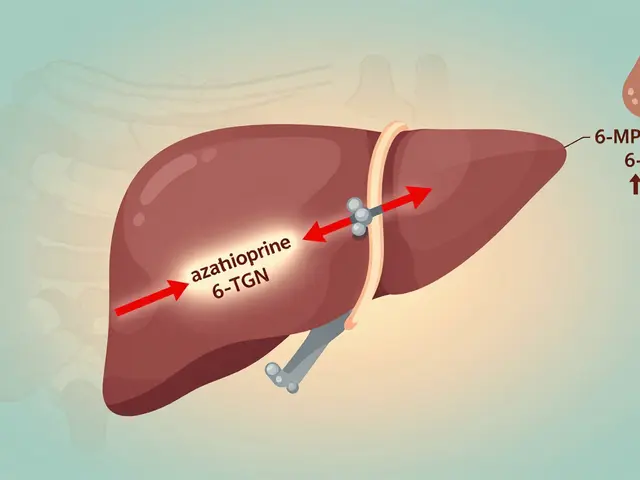
Azathioprine and Allopurinol: How Low-Dose Combination Therapy Prevents Toxic Metabolite Buildup
LDAA therapy combines low-dose azathioprine with allopurinol to redirect toxic metabolite production toward therapeutic effects. It’s a proven solution for patients with high liver enzymes or poor response to standard thiopurine therapy, but requires strict monitoring to avoid bone marrow suppression.

How to Wear a Medical Alert Bracelet for Severe Drug Allergies
Wearing a medical alert bracelet for severe drug allergies can save your life in an emergency. Learn what to engrave, where to wear it, and why it's the most reliable way to tell first responders what you're allergic to.

Managing and Preventing Side Effects of Isotretinoin
Isotretinoin is a powerful acne treatment but can come with a slew of side effects. This article explores practical ways to manage and prevent these effects, helping users navigate their treatment with confidence. Learn about dietary adjustments, skincare routines, and lifestyle changes that can mitigate potential issues. Understand when to consult your doctor and how to recognize serious side effects. Empower yourself with the right knowledge to balance treatment success with minimized discomfort.